To create a report of the Medical record of a patient, use CCR/CDD submenu under EHR Advanced menu. The CCR/CCD can be shared between providers and to the patients.
About CCR
The Continuity of Care Record (CCR) is a health record standard specification developed jointly by ASTM International, the Massachusetts Medical Society(MMS), the HIMSS, the American Academy of Family Physicians (AAFP), the American Academy of Pediatrics (AAP), and other health informatics vendors.
The CCR standard is a patient health summary standard. It is a way to create flexible
documents that contain the most relevant and timely core health information about a patient,
and to send these electronically from one care giver to another. It contains various
sections such as patient demographics, insurance information, diagnosis and problem list, medications, allergies and care plan. These represent a “snapshot” of a patient’s health data that can be useful or possibly lifesaving, if available at the time of clinical encounter. The ASTM CCR standard is designed to permit easy creation by a physician using an electronic health record (EHR) system at the end of an encounter.
Because it is expressed in the standard data interchange language known as XML, a CCR can potentially be created, read and interpreted by any EHR or EMR software application. A CCR can also be exported in other formats, such as PDF.
Search Filters in CCD/CCR Report
| Field | Description |
| Patient | Provide Name or MR# |
| Date | Provide the date range for which the report is to be generated |
| Document Type | Select one from the drop-down: Continuity of Care Document/Referral Note/Discharge Summary |
Search Screen of CCD/CCR Report
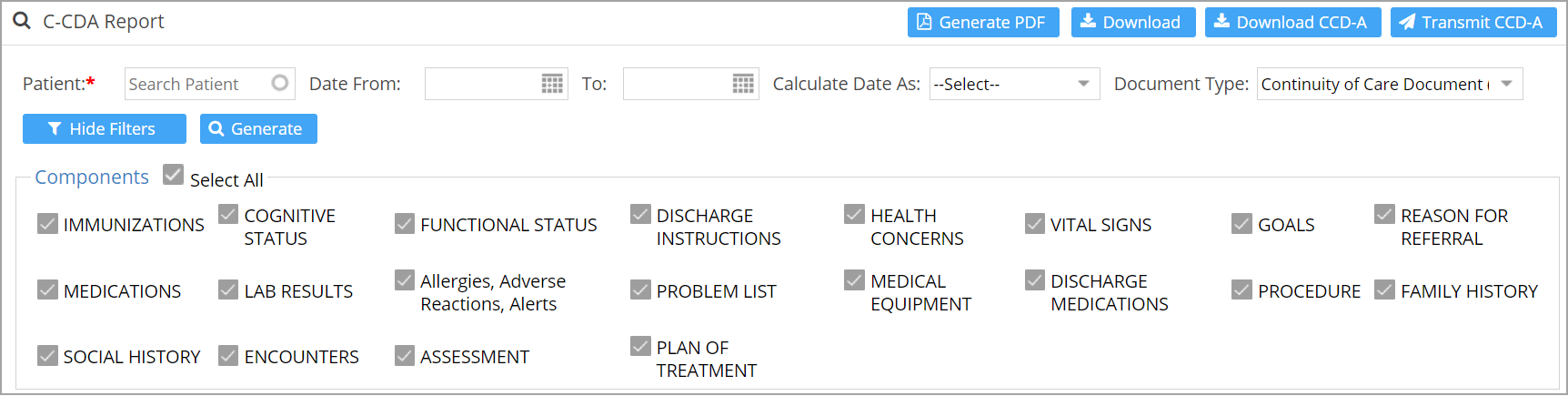
Note: By default all Components are checked. Uncheck the items not required.
Report Generation
| Field | Description |
| To generate the PDF output which can be mailed or printed and given to patient | |
| To download as html file | |
| To download as xml file | |
| To fax the report as either xml or html |
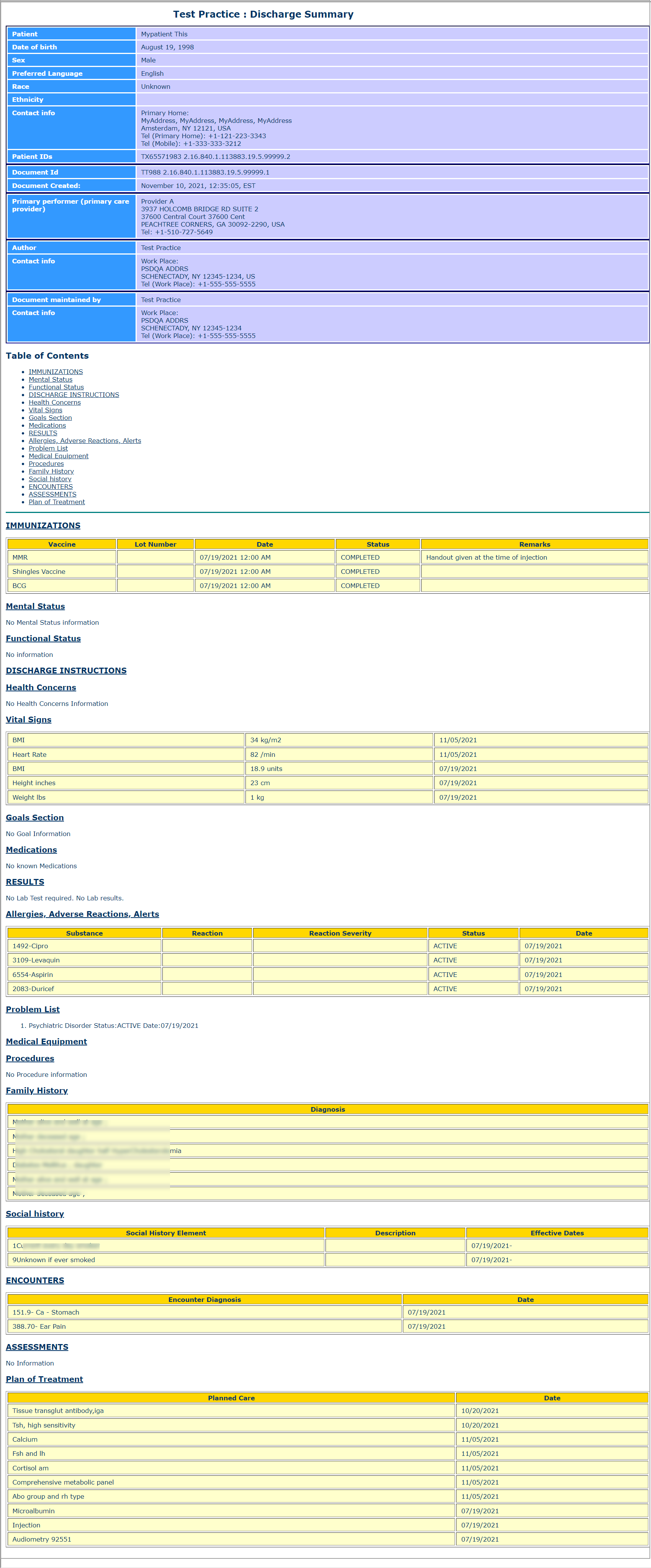
Sample Report